I wonder if it is because more older people are now vaccinated but they aren't doing it for kids yet? Not young ones anyway. But that would be especially bad given the long term health problems. The recent research on what it does to the brain is very troubling. We're in for a world of pain if it hits the young and causes long term health problems. Especially with the shit healthcare system in the US and the lack of solid healthcare in so much of the world.
From what I understand, it's related to the lower vaccination rates of younger people. Full vaccination is still doing its job with delta (most recorded break-through infections in Canada were asymptomatic or very mild - there was one death though, but an 80 y.o. with serious comorbidities).
In the window of a vintage shop in the Sydney suburb of Annandale, a sign expresses the frustration of many Australians with their country's pandemic strategy.
"People cannot feel safe just because they had the two doses," said the assistant director-general for access to medicines and health products at the WHO.
My work has been very tight-lipped about its reopening plan, and really has been pretty "let's not talk about the unpleasantness" about the pandemic in general. Every announcement since last March has boiled down to "we're trying to figure out reopening, but you are free to work from home until [insert some month 2-6 months from now]." Our office culture is very in-person, community-oriented (it veers on forced fun at times), and a lot of people are itching to get back in.
I have a few coworkers whose productivity has dipped in the last 15 months and have requested to start working from the office once more. I'm on the opposite end and honestly feel no real rush to get back into the office; I like that I have more control over my time, and it's been easier to develop healthy habits re: food and exercise. Yesterday our department head pulled us into zoom with a reopening announcement which was "we don't have a plan, but we want a hybrid model and won't be truly reopening the office until December." All employees who do want to work in the office can get in touch with their manager to make arrangements. If I want to go back to the office I'll need to take the initiative and come up with a plan that suits me, advocate for what equipment I need or want.
My company is also overwhelmingly religious in makeup (it's not uncommon to see people share messages of hope from the LDS in Slack), and I think there may be many who don't actually want to vaccinate. There's no indication of whether we'd need to be masked in office, or if they're requiring vaccination in order to return to the office. I honestly don't trust some of these people but I'm nervous to push back and request that management express a clear stance on masking and vaccination in the workplace.
Which, to me, feels like a microcosm of how the entire country is handling this thing. My county is opening up as of yesterday, and masks aren't required. I went into the corner store today and the staff was unmasked, but many shoppers were. It's been left up to the individual to decide what they consider risky, what level of risk they want to expose themselves to, and in what capacity they'll mitigate that risk. It feels like we're back in February 2020 and we've learned nothing from this massive tragedy. We're just whistling past the graveyard for the foreseeable future.
CNN had a story about the 10 things we learned from COVID travelers this year
Not surprisingly, many people from around the world are traveling to the united states to get a jab. Most often while on vacation on an Island or Territory of the United States.
Another article states that for many republicans, not getting a vaccine is considered a badge of honor.
So we have people traveling from around the world to the US to get COVID vaccinations and many of our own citizens who do not want them.
I just heard that lying to your SO over your vaccination status is a thing.
A couple weekends my mother went camping at the Pocono Raceway for the NASCAR race. My mother and step father shared a RV with one of his best friends. Who also brought along his girlfriend, daughter and her husband.
The topic came up of raise your hand if you have been vaccinated and only my mother's hand went up. My step fathers friend was like "we don't believe in the vaccine at our house."
Later that night, my step fathers friends girlfriend confided in my mother that she in fact has been vaccinated. She has to be to visit high risk family members. But she can't openly say or admit to her SO that she has been vaccinated because he is so against it.
Norwegian Cruise Line Holdings is suing Florida's surgeon general over the state's law that prohibits companies from requiring customers and employees to provide documentation of Covid-19 vaccination status.
Norwegian Cruise Line Holdings is suing Florida's surgeon general over the state's law that prohibits companies from requiring customers and employees to provide documentation of Covid-19 vaccination status.
My thoughts on this are that they kinda had to do this. It's entirely reasonable for a private company to restrict passengers to those that are vaccinated. Forcing them to take unvaccinated passengers would open them up to all sorts of litigation if someone gets very sick and dies of Covid because they did not check vaccination statuses. IMHO, this was the only reasonable answer to the law.
Children will likely pay the price for adults in the US not getting vaccinated at high enough rates to slow or stop the spread of Covid-19, which has been surging in most states, a vaccine expert said.
Children will likely pay the price for adults in the US not getting vaccinated at high enough rates to slow or stop the spread of Covid-19, which has been surging in most states, a vaccine expert said.
The article headline came up different than what it was on CNN. But basically the part that has me really worried is that up to 30% of children who become infected by covid / delta may become covid long-haulers. And that is very alarming.
The article headline came up different than what it was on CNN. But basically the part that has me really worried is that up to 30% of children who become infected by covid / delta may become covid long-haulers. And that is very alarming.
We've been diving into Covid long hauler data and our findings have been consistent with others in that, it seems to affect the body for about 3 months before symptoms fade for most patients.
First here's a great synopsis of what "long Covid" really is: “Long COVID” is a term used to describe presence of various symptoms, even weeks or months after acquiring SARS-CoV-2 infection irrespective of the viral status [8]. It is also called “post-COVID syndrome”. It can be continuous or relapsing and remitting in nature [9]. There can be the persistence of one or more symptoms of acute COVID, or appearance of new symptoms. Majority of people with post-COVID syndrome are PCR negative, indicating microbiological recovery. In other words, post COVID syndrome is the time lag between the microbiological recovery and clinical recovery [10]. Majority of those with long COVID show biochemical and radiological recovery. Depending upon the duration of symptoms, post COVID or Long COVID can be divided into two stages-post acute COVID where symptoms extend beyond 3 weeks, but less than 12 weeks, and chronic COVID where symptoms extend beyond 12 weeks
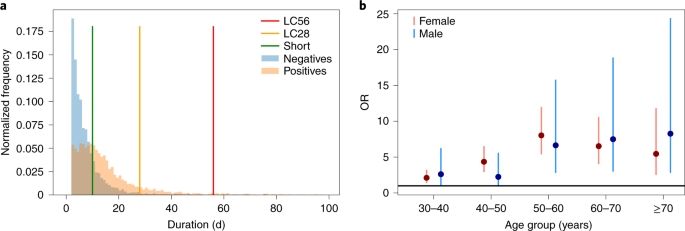
Risk factors: Follow up of patients recovered from COVID identified a few factors which are commonly associated with development of long COVID. The risk of long COVID is twice common in women compared to men [9]. Increasing age is also a risk factor and it is found that patients with long COVID are around four years older than those without [9]. Presence of more than 5 symptoms in the acute stage of illness is associated with increased risk of developing long COVID [20]. Symptoms most commonly associated with long COVID include fatigue, headache, dyspnea, hoarse voice and myalgia [20]. Presence of co morbidities also increases the risk of developing post COVID syndrome. Even those with mild symptoms at initial presentation were noted to develop long COVID.
Long COVID is the collective term to denote persistence of symptoms in those who have recovered from SARS-CoV-2 infection. WE searched the pubmed and scopus databases for original articles and reviews. Based on the search result, in this review ...
www.ncbi.nlm.nih.gov
This article mainly looks at hospitalized people and their long covid, but in the general population, we are seeing symptoms fade for most people, because most people do not fall in the risk group stated above.
Some articles are tagging long hauler covid as being at about a 10% prevalence in the population that contracted covid.
Overall, approximately 10% of people who’ve had COVID-19 experience prolonged symptoms, a UK team estimated in a recently published Practice Pointer on postacute COVID-19 management. And yet, the authors wrote, primary care physicians have little evidence to guide their care. As Their Numbers Grow, COVID-19 “Long Haulers” Stump Experts
But when we start actually slicing and dicing this into days (or weeks) post infection, we see that there are drop offs (at least in the data we're looking at) in symptoms from 60 to 90 to 120 days. I really like the way this analysis breaks it down.
We analyzed data from 4,182 incident cases of COVID-19 in which individuals self-reported their symptoms prospectively in the COVID Symptom Study app1. A total of 558 (13.3%) participants reported symptoms lasting ≥28 days, 189 (4.5%) for ≥8 weeks and 95 (2.3%) for ≥12 weeks.
Analysis of data from the COVID Symptom Study app reveals fatigue, headache, dyspnea and anosmia as key attributes of long COVID, with those experiencing five or more symptoms during the first week of being at increased risk of prolonged disease.
www.nature.com
And while there are reports of Covid harming organ tissue, it seems to get better as time goes on--or the difference between microbiological recovery and clinical recovery--as long as the person isn't in one of those risk groups with the comorbid conditions.
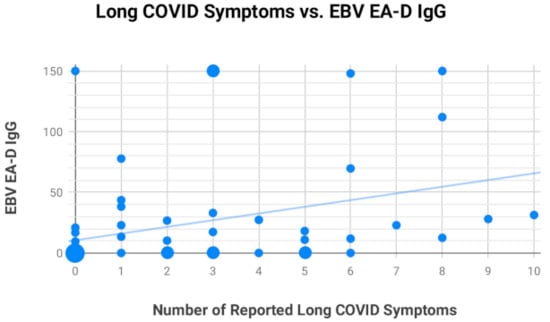
As an aside, this study suggests that Epstein–Barr virus (EBV)
We found the prevalence of long COVID symptoms to be 30.3% (56/185), which included 4 initially asymptomatic COVID-19 patients who later developed long COVID symptoms. Next, we found that 66.7% (20/30) of long COVID subjects versus 10% (2/20) of control subjects in our primary study group were positive for EBV reactivation based on positive titers for EBV early antigen-diffuse (EA-D) IgG or EBV viral capsid antigen (VCA) IgM. The difference was significant (p < 0.001, Fisher’s exact test). A similar ratio was observed in a secondary group of 18 subjects 21–90 days after testing positive for COVID-19, indicating reactivation may occur soon after or concurrently with COVID-19 infection. These findings suggest that many long COVID symptoms may not be a direct result of the SARS-CoV-2 virus but may be the result of COVID-19 inflammation-induced EBV reactivation.
Coronavirus disease 2019 (COVID-19) patients sometimes experience long-term symptoms following resolution of acute disease, including fatigue, brain fog, and rashes. Collectively these have become known as long COVID. Our aim was to first determine long COVID prevalence in 185 randomly surveyed...
www.mdpi.com
So, is this scary? Yes. But, there are still a lot of things we don't know about this virus. Don't worry too much. We have been finding that most people that are healthy tend to recover. It might take a while, but they do recover. Just like the myocarditis that the vaccines were causing, researchers found that the organ damage was only temporary for a majority of the young men who had this side effect.
But also, don't be dumb. The delta variant is here, so maybe consider social distancing, masking, and avoiding large gatherings.
Jill Filipovic writes that the danger inherent in ideological partisan divides over Covid-19 vaccination is evident in Tennessee, where the firing of Dr. Michelle Fiscus reinforces the enduring irony that the GOP, the "pro-life" party, doesn't believe that children, including teens, have basic...
www.cnn.com
A doctor in Tennessee doctor sent out a memo about what to do if a minor shows up for a vaccination without their parents consent. She covered the minor doctrine.
She was fired for sending out the memo. She was accused of undermining the authority of parents.
The governor gave her a choice, resign or be terminated as she is a public health official.
All 50 states are seeing a surge in covid cases post 4th of July weekend.
This is being attributed to everyone throwing all precautions to the curb once it was no longer required by the government and low vaccination rates in several states.
States with low vaccination rates are seeing 4 digit percentage increases in covid in several counties.
People just want back to normal to fast and the virus hasn't been beaten yet do to getting the vaccine becoming politicized.
All 50 states are seeing a surge in covid cases post 4th of July weekend.
This is being attributed to everyone throwing all precautions to the curb once it was no longer required by the government and low vaccination rates in several states.
States with low vaccination rates are seeing 4 digit percentage increases in covid in several counties.
People just want back to normal to fast and the virus hasn't been beaten yet do to getting the vaccine becoming politicized.
Yeah, there's an event that's been on hiatus since the pandemic in Atlanta called Controllerize, I always wanted to go. Low-fi Hip Hop DJ's, Video Games, Anime, Artists, all at Monday Night Brewery. They had their first day back last week, 700+ attendees, no masks that I saw in any of the pictures, and of course there was a COVID outbreak.
If people would just get vaccinated and chill out we'd be fine, but everyone is impatient and stubborn.
But hey, some 24 year old with no underlying health conditions just needed a double lung transplant from catching COVID, so, you know, it's not a big deal if you're young and healthy, right? Right?
All 50 states are seeing a surge in covid cases post 4th of July weekend.
This is being attributed to everyone throwing all precautions to the curb once it was no longer required by the government and low vaccination rates in several states.
States with low vaccination rates are seeing 4 digit percentage increases in covid in several counties.
People just want back to normal to fast and the virus hasn't been beaten yet do to getting the vaccine becoming politicized.
I was on a call with colleagues and we were discussing Covid--specifically the covid reporting we do in my organization--and right now in Jacksonville, they are cancelling elective surgeries in hospitals there. What does this mean? It means that hospitals are starting to fill up again with Covid patients and it looks like they are, yet again, starting to displace routine medical procedures due to lack of space and precaution. I do not expect another lock down, especially not in red states. But this thing is far from over.
With Covid-19 cases rising in all 50 states, health officials say it's clear that unvaccinated people are both driving the increase in cases and are most at risk.
www.cnn.com
Also in the news is LA County has issued a mask mandate again.
I suspect any more restricts have long sailed away in many red states, but I suspect we may see some return in blue states.
Will be interesting to see if the CDC / federal government enacts any restrictions and if they do will red states follow or ignore.